 ACLS and BLS Lecture Notes:
In this video, we will delve into the protocols for responding to cardiac arrest, both non-shockable and shockable rhythms, as well as symptomatic bradycardia. By following the American Heart Association's algorithms, you will gain a clear understanding of the essential steps to take in these critical situations.
In conclusion, Immediate recognition and intervention are crucial in cardiac arrest or symptomatic bradycardia. The sooner treatment is administered, the higher the chances of positive outcomes. By following these ACLS guidelines, you will be well-equipped to confidently respond to cardiac emergencies and improve patient outcomes.
0 Comments
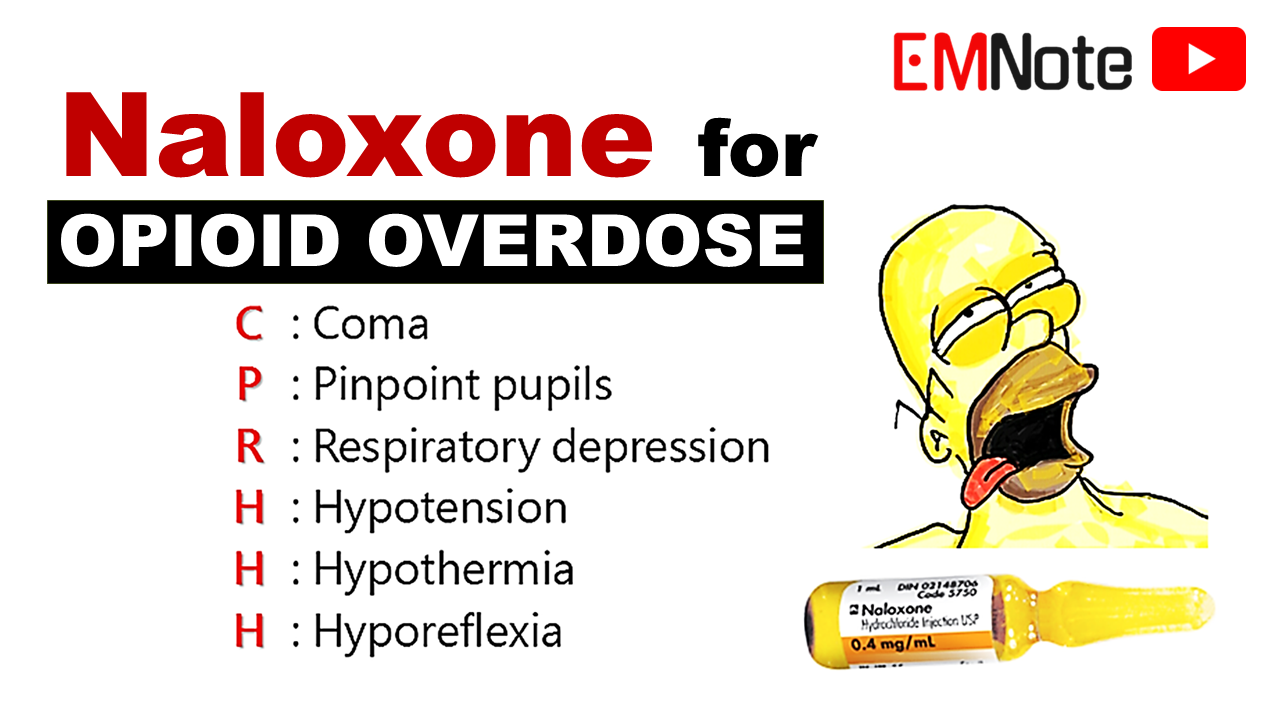  When and How to Administer Naloxone?
Here are the preparations you'll need for diluting naloxone:
To dilute naloxone, follow these instructions:
Summary:
 Pitfalls in Difficult Airway Management
📌Pre-intubation Risk Assessment:
📌Avoid Inappropriate Ventilator Settings:
📌Avoid Unnecessary Sodium Bicarbonate.
📌Avoid Prolonged Apnea.
📌Avoid Post-intubation Hypotension.
📌Avoid Inappropriate Induction Agents and Doses.
📌Conclusion
 Neonatal Resuscitation in the Delivery Room
Term, Tone, and Tantrum Assessment:
Delayed Cord Clamping:
Prompt Resuscitation for Neonates:
Avoid Routine Bulb Suctioning:
Positive Pressure Ventilation:
Chest Compressions and Epinephrine:
Consider Blood Loss and Pneumothorax:
 Post-cardiac arrest care
- Four key areas: - Blood pressure support - Immediate catheterization - Targeted temperature management - Full-body imaging Blood pressure support - If SBP below 90 or MAP below 65 mmHg - Initial treatment: 1-2 liters of IV saline or Lactated Ringer's - Vasopressors if BP remains low - Norepinephrine for non-arrest patients - Dopamine, vasopressin, and phenylephrine as second-line agents - Epinephrine for severe hypotension or last resort Immediate catheterization - ST-elevation myocardial infarction (STEMI) patients: immediate PCI - Non-STEMI patients: - Observational studies suggest potential benefits - Randomized controlled trials show mixed results Targeted temperature management (TTM) - Therapeutic hypothermia at 33°C initially recommended - TTM2 trial: no significant difference between 33°C and 36°C - Maintain core body temperature between 32°C and 36°C for at least 24 hours - Trained professionals for induction and monitoring Full-body imaging - Reveals important findings in some cases - Routine use of extensive imaging controversial - Further research needed to determine true benefit Conclusion - Complex decision-making in post-cardiac arrest care - Stay informed on evolving evidence and guidelines - Provide optimal care to patients following a cardiac arrest event |

Author
|